June 2024 - Case of the Month
Angelle M. Jolly, MD, Bushra Nazir, MD
A male patient in his mid-30s with a history of hypertension presented multiple times
to the emergency department due to worsening odynophagia and gingival bleeding following
a dental procedure. His condition continued to worsen, and he was subsequently admitted
due to requirement for intravenous (IV) antibiotics. On admission, he was incidentally
found to have significant leukocytosis (34.9 x 103/µL), as well as anemia (hemoglobin: 10.5 g/dL) and thrombocytopenia (platelets: 106
x 103/µL). A peripheral blood smear was reviewed and revealed 16.0% blasts with rare Auer
rods and 13.0% promonocytes (Figure 1).
Considering the abnormal peripheral smear, the Hematology and Oncology team was consulted,
and a bone marrow biopsy was performed. The aspirate (Figure 2) and core biopsy (Figure
3) were found to be hypercellular (core biopsy cellularity of 80%) with increased
blasts and promonocytes. A manual count of the aspirate yielded a blast count of 15.0%
and a promonocyte count of 28.0%. Together, blasts and promonocytes were a total of
43.0% on manual count.
Bone marrow flow cytometry revealed approximately 63.0% cells with monocytic differentiation.
These cells were positive for CD4 (dim to moderate), CD13 (subset, dim), CD14 (heterogenous),
CD33 (dim), CD34 (subset, dim), CD64 (dim to moderate), CD117 (subset, dim), HLADR
(subset, moderate) and myeloperoxidase (MPO).
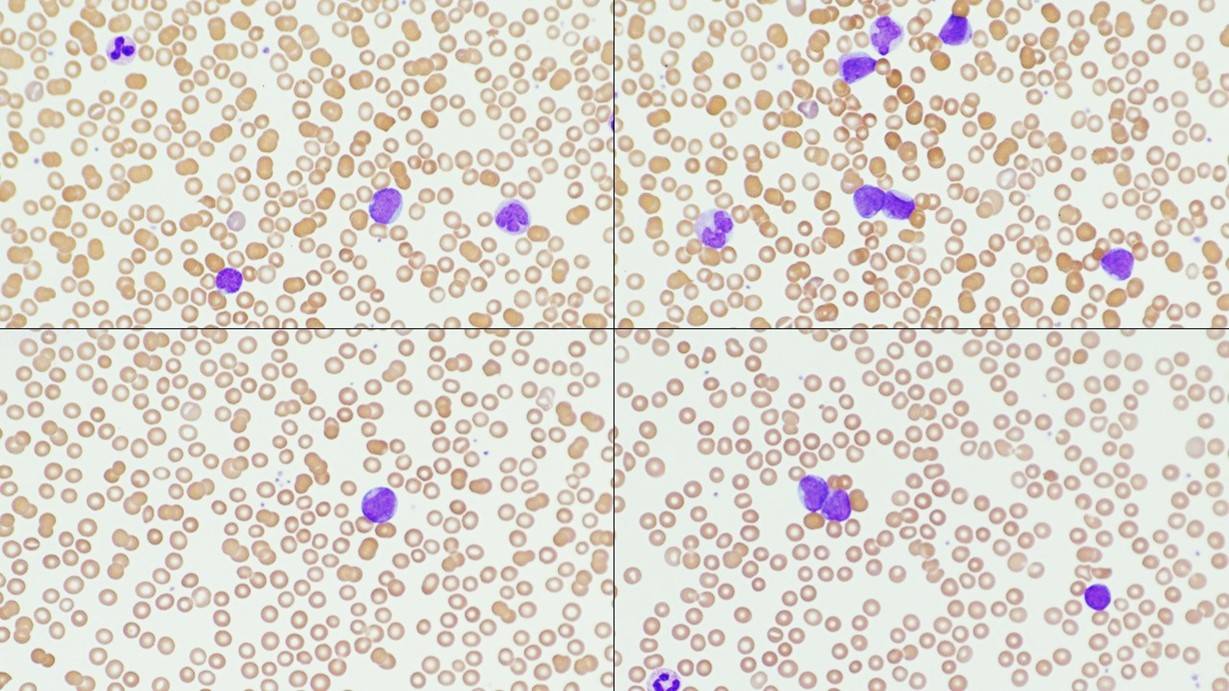
Figure 1
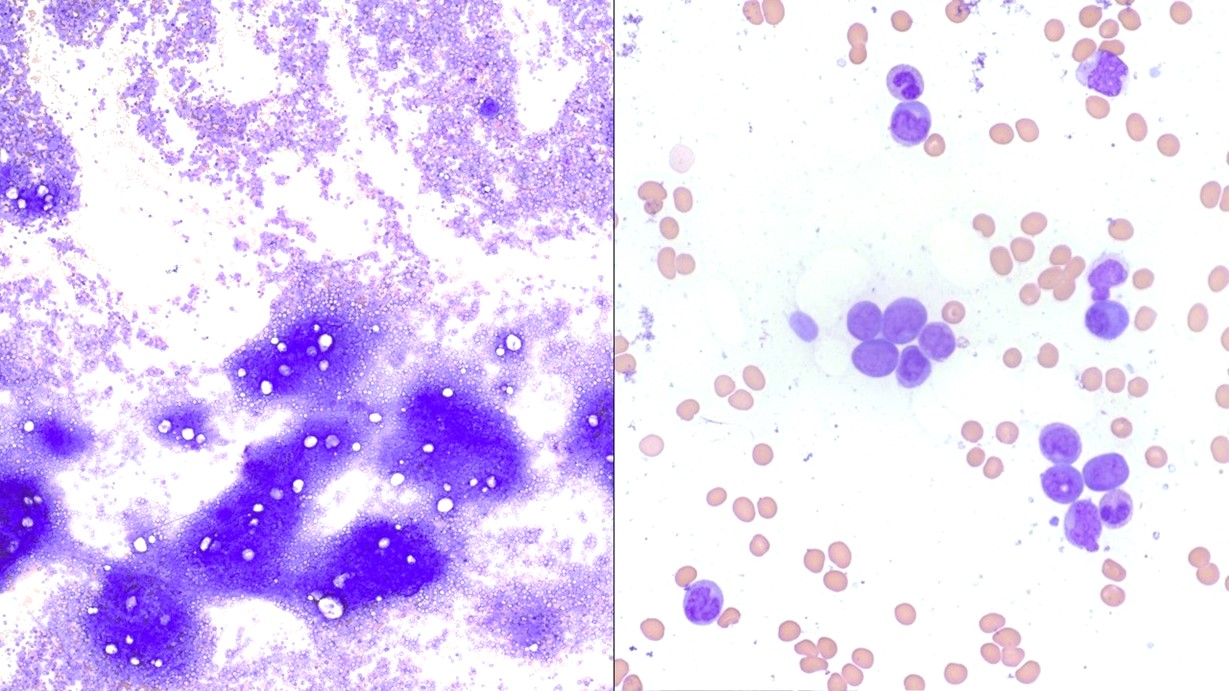
Figure 2
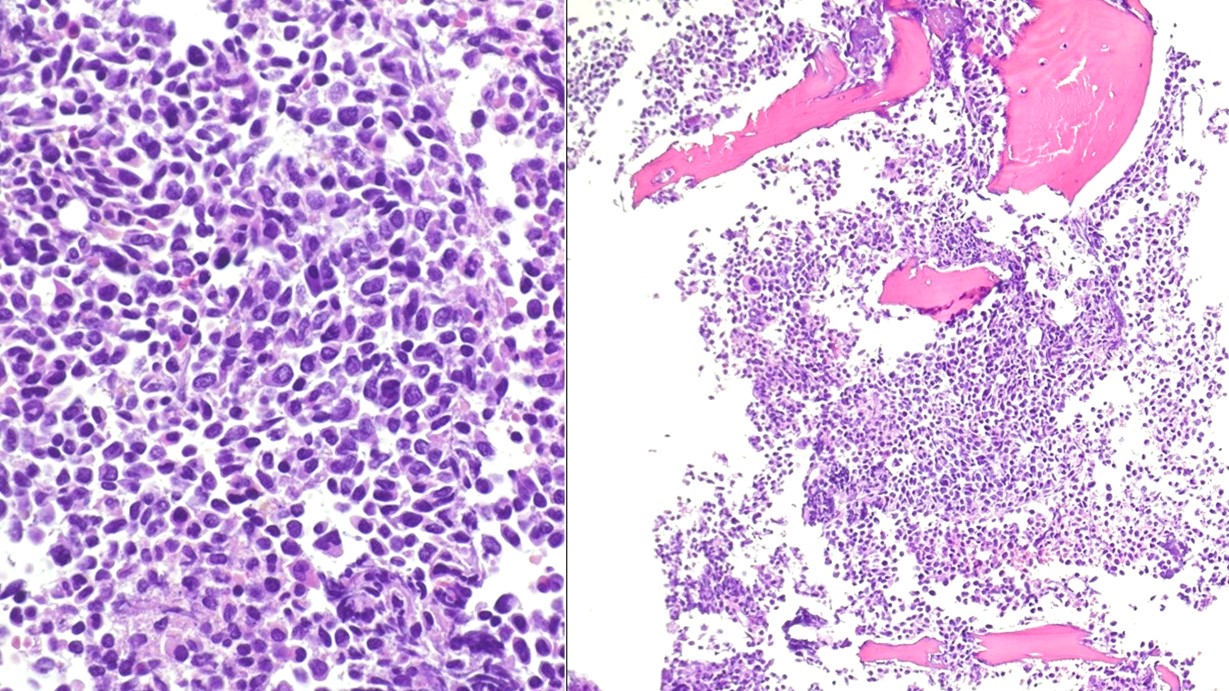
Figure 3
Question: What next step in the workup is most likely to yield the correct diagnosis for this
patient?
A. No further workup is required
B. Fluorescence in situ hybridization(FISH) studies for an acute myeloid leukemia
(AML) Panel
C. Solid tumor panel by next generation sequencing (NGS) studies
D. Molecular testing for a JAK2 mutation