October 2023 Case
Contributors: Ayesha Younus MBBS, Zhiyan Fu MD, MS, Shaun Lawicki MBBS
Clinical History and Presentation
A young woman in her 20’s presented with a one-week history of worsening abdominal pain, nausea, fatigue, intermittent fevers and chills, lightheadedness, weakness, and dark urine. She was diagnosed with a urinary tract infection and discharged on oral antibiotics.
She presented to the emergency room (ER) 4 days later due to no resolution in her previous symptoms, and her abdominal pain is now more localized to the right upper quadrant. Past medical history is significant for flu-like symptoms a week prior, but no significant underlying illnesses or previous hospital admissions or surgeries. She denied any recent exposure to freshwater, international travel, or intravenous drug use. Family history was significant for psoriasis in her mother and rheumatoid arthritis in her grandmother.
Upon physical examination, she appeared obese and had tenderness in the right upper quadrant of her abdomen. Her skin and sclera were jaundiced. Imaging studies showed mild hepatomegaly with steatosis and mild splenomegaly.
Laboratory Results are as follows:
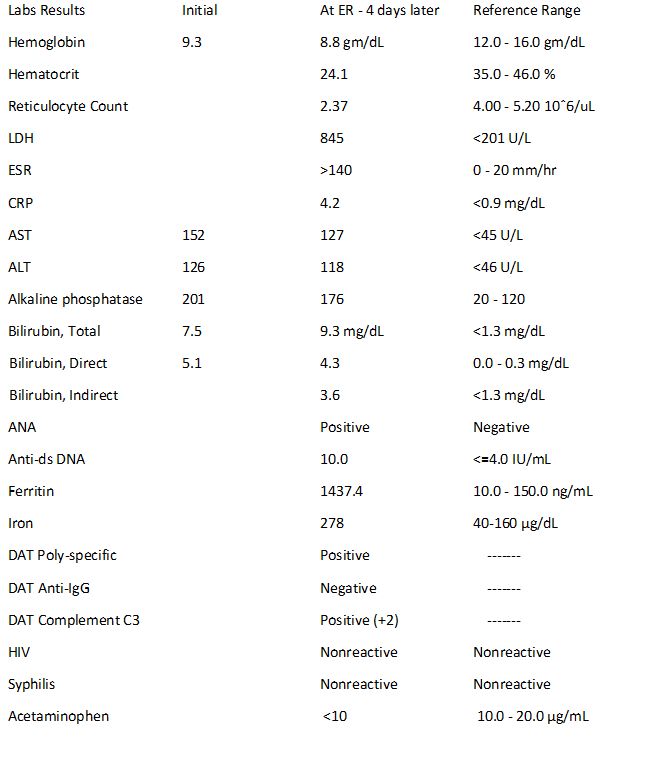
Acute hepatitis panel was negative at both presentations.
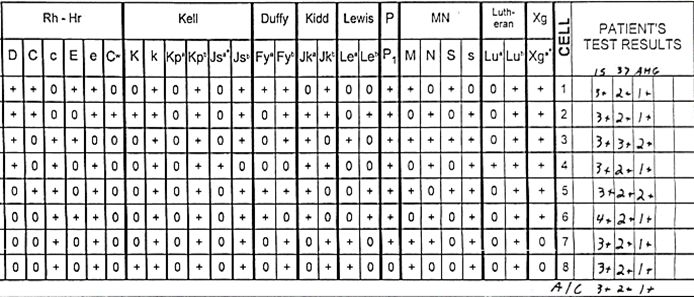
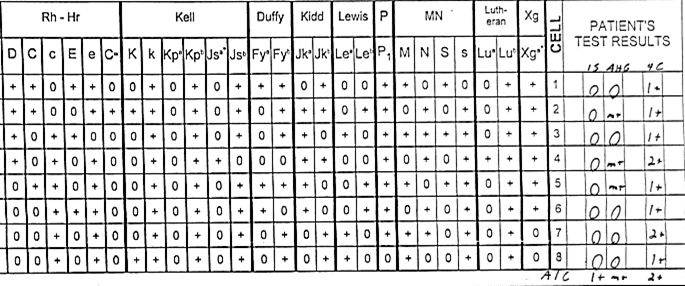
Blood Bank Testing:
Patient is O+. At the initial presentation, panreactivity was seen at all phases of tube testing – Immediate Spin (IS); 37oC; and Anti-Human Globulin (AHG) with reagent cells and with the patient’s own cells (Auto Control). Rabbit erythroid stroma (RESt) adsorption removed the panreactivity.
At the ER presentation 4 days later, antibody screening using automated solid phase testing was negative. Tube testing revealed no reactivity at IS but microscopic (m+) positivity at AHG with ~1/3 of reagent cells. Additional testing at 4oC revealed 1-2+ panreactivity. Prewarming removed all reactivity. The Autocontrol (AC) was 1+ at IS and m+ at AHG. The Direct Antiglobulin Test (DAT) was 2+ Polyspecific, (Poly). The two components of the Poly reagent, Anti -C3d Complement (C3) and IgG were 2+ positive (C3) and negative (IgG) respectively.
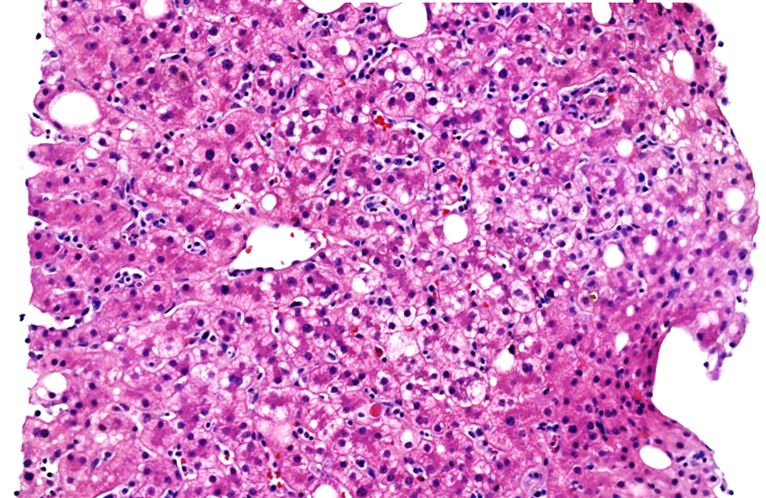
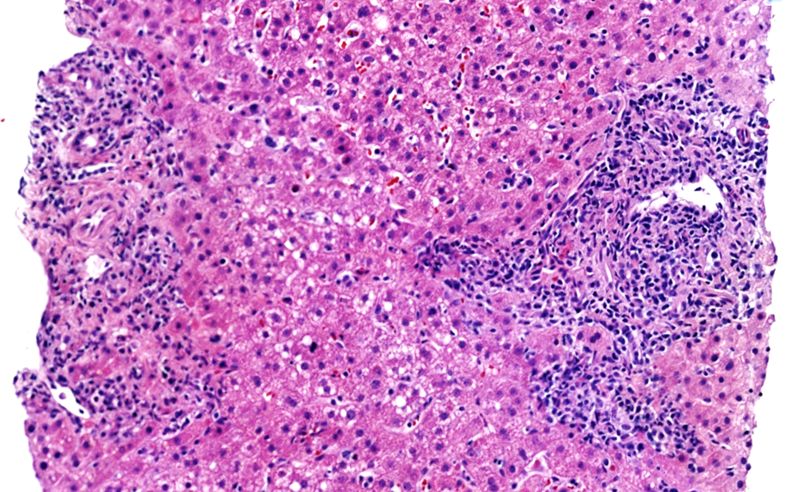
A liver biopsy was performed, representative images are below:
What is the most likely cause of the patient’s condition?
- Autoimmune hepatitis
- Lymphoproliferative disorders
- Acute infectious hepatitis
- Drug-induced liver injury